What are the GI surgeries that I should be ready to perform?
Intestinal biopsies (covered in the Exploratory Laparotomy session)
Gastrotomy
Enterotomy
Resection and anastomosis (RnA)
Situational Awareness
Not every veterinarian is comfortable doing a GI surgery because of the potential severity of complications (such as dehiscence) and the difficulty in obtaining sufficient experience with the variable situations that can arise.
The truth is that an enterotomy and a gastrotomy are relatively easy procedures with a low complication rate, and both are often life saving. As a result, the general practitioner needs to be ready to perform these procedures, and should not hesitate to do so.
The RnA can be more daunting but the principles are similar. There are also a few more steps to remember and the procedure will take more time. But once you have determined that a loop of bowel is not viable, you must proceed with the RnA. Be prepared (watch the video before entering the OR) and just do it!
If you have a significant aversion to the RnA, then you need to practice good case selection by recognizing the cases that most likely require the procedure (for example: longer duration, more severe symptoms/metabolic changes, free fluid/bacteria in the abdomen). These cases should then be referred.
$375
Get ready to perform a GI surgery:
All the information you need.
Fully narrated surgical videos.
In depth guide and more.
Imaging of the abdomen, preferably ultra sound but survey radiographs (2 views) are a good start.
Urinalysis
What the client needs to know:
The length of the recovery is proportional to the amount of tissue damage.
The cost of the procedure is proportional to the amount of tissue damage.
The amount of tissue damage is proportional to the duration and severity of the problem.
Step by Step Gastrotomy
Figure G1
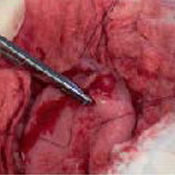
Pack stomach from abdomen with moistened lap sponges; Use stay sutures to hold the stomach up; make a stab incision in the least vascular portion of the body of the stomach.
Figure G2
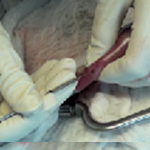
Enlarge the size of the gastrotomy incision using mayo or Metzenbaum scissors; insert a finger or the entire hand to retrieve FB(s)
Figure G3
Change gloves and close the gastrotomy. I start with a full thickness simple continuous.
Figure G4
I then double back over my suture line with a continuous inverting pattern, Cushing (as seen here) or Lembert.
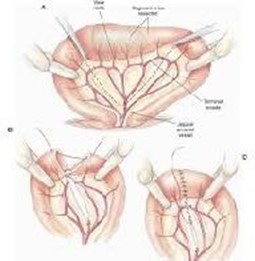
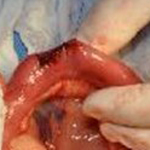
Figure RNA1
This picture is just here as a reminder of the important steps of the RnA. Please watch the course video for a full understanding of this surgery.
Exteriorize the affected loop of bowel from the abdomen, pack off with moistened lap sponges and place the doyens. Place Criles or Kellys on the section of bowel to be removed. Ligate the appropriate vessels (including the ones along the mesenteric border of the bowel). Excise the affected portion. Suture the remaining bowel, end-to-end with a simple interrupted, apposing (not crushing) pattern using 3-0 or 4-0 absorbable monofilament suture. Leak test, change gloves/instruments, lavage, close rent in mesentery and close abdomen.
Step by Step Enterotomy
Step by Step Enterotomy
Figure G1
Exteriorize the affected loop of bowel and pack it off with moistened lap sponges. Place doyens onto healthy bowel on either side of FB.
Figure G2
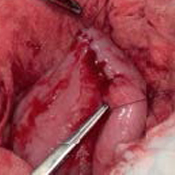
If the FB is can be moved within the bowel then incise aborad of the FB; if the FB can not be moved, then incise over the FB, and towards the stomach (orad).
Figure G3
Enlarge the incision in the bowel with Metzenbaums.
Figure G4
Suture the enterotomy site closed with a simple interrupted, apposing but not crushing, pattern, short lasting absorbable monofilament (3-0 or 4-0). Start in the centre of the incision.
Get ready to perform a GI surgery:
Preferred instrumentation:
Abdominal retractors
Doyen
Lap sponges
3-0 or 4-0 monocryl for the GI
Warm saline for flushing
Suction with Poole or Yankhaur suction tip
Second set of instruments and gloves for closing
Post-operative Considerations:
Anti-emetics (Cerenia)
Appropriate pain management
Antibiotics (duration based on perceived level of contamination)
NPO for 8-12 hours
Start with water and then small meals
Adjust diet if necessary
What you get when you register:
A comprehensive list of instruments
A step-by-step narrated pictorial description of how to perform a gastrotomy, enterotomy and RnA.
Fully narrated videos for each of those surgeries
Tips and tricks for easily and successfully performing those surgeries
Information on how to assess the bowel and what to do if you are uncertain
Information on how to manage a string foreign body
A discussion on diagnostics
How to minimize tissue and patient trauma while you are performing these surgeries
Case selection to help keep the stress level down
What types of cases may not actually need your help.
Q & A
How should an enterotomy be closed?
The simple interrupted apposing (not strangulating) suture pattern with a shorter-acting, absorbable, monofilament material (MonocrylTM) works well and is simple. I like to use 4-0 in a small patient and 3-0 in a larger patient; select a taper point needle if you can; I like the SH needle. I tend not to use 2-0 on the bowel, I find it too large, but I know some surgeons who do use the larger suture and have success; so select a size you are comfortable with. I recommend you leak test all your enterotomy closures.
How should a gastrotomy be closed?
The stomach heals well and can be closed in a variety of ways. My preference is a 2 layer closure with a simple continuous full thickness closure followed by a continuous inverting, non-full thickness, pattern (Lembert or Cushing). I select a shorter acting absorbable monofilament (MonocrylTM). I tend to use a 3-0 on the smaller patient and 2-0 on the larger ones for the stomach. I would suggest avoiding the simple interrupted pattern here; the continuous pattern offers a better seal and is faster to perform, the gastrotomy is often a longer incision.